 |
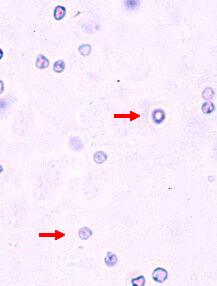
The arrows
indicate red blood cells. Observe the absence of a granular texture as well as absence of a nucleus in these cells. In the lower red blood cell, notice the characteristic biconcavity reflected by a central denisty (depression). |
Your diagnosis
|
Diagnosis and comments by the pathologist CBC : The changes observed are compatible with a stress leukogram (a neutrophilia without left shift or the presence of toxic neutrophils, lymphopenia and eosinopenia). A differential diagnosis for the neutrophilia includes an inflammatory process which can be excluded by the clinical signs, physical exam and other relevant information. Clinical chemistry : The chemistry changes observed combined with the specific gravity and response to fluid therapy are compatible with renal failure. The mixed acid-base disorder can be explained by the vomiting that causes metabolic alkalosis; this can be derived from the large difference between the chloride and sodium values which exceeds 45 mmol/L; a high anion gap metabolic acidosis is caused by circulating organic acids that 1- have accumulated due to renal failure which prevents their excretion (metabolic waste products) and 2- that are exogenous (see below). Urinalysis : The crystals (here magnified to 1000X) are calcium oxalates (monohydrate). In small quantities in a urinary sediment (one or two crystals visible in rare cases), they aren't necessarily always significant. But in larger quantities, they are highly suggestive of an ethylene glycol toxicity. This product, commonly found in commercial antifreeze, is metabolized by the liver and leads to the formation of oxalates that precipitate with calcium in the renal tubules and are then eliminated in the urine. Note that crystals aren't always found in ethylene glycol toxicity (urinalysis done before or after the crystals' passage into urine). Also, depending on the moment when the animal is examined and the amount of antifreeze ingested, another clinical chemistry change which may be observed is hypocalcemia (the calcium is chelated by ethylene glycol metabolites). In this case, the proteinuria can be caused by two things: 1-presence of blood in urine ; however, the amount is small (1+), or 2- a glomerular lesion. In samples collected by cytocentesis, it's common to find blood in the urine. Confirmation for proteinuria of glomerular origin or confirmation of hematuria should ideally be done from a sample collected by free catch. Comments: In some cases of ethylene glycol toxicity, the acidosis can be severe. The diagnosis of ethylene glycol toxicity requires a look at several factors, such as the patient's history (that can reveal information about in-house or garage activity; places where the animal has had access to in the previous days), the clinical signs (weakness, ataxia or other CNS signs, signs associated with renal failure), and variable clinical chemistry findings depending on when the animal is presented. The same applies to urinalysis results. Final diagnosis : Ethylene glycol toxicity |
|
The arrows
indicate red blood cells. Observe the absence of a granular texture as well as absence of a nucleus in these cells. In the lower red blood cell, notice the characteristic biconcavity reflected by a central denisty (depression). |